Research has shown that there is a relationship between a woman’s vitamin D status and the success rates of assisted reproduction therapy(ART), which includes IUI, IVF and ISCI.
While this is research is nothing new, and something I have been promoting for years, finally it is now official. Women trying to conceive should be taking vitamin D supplements, eating vitamin D rich foods, and getting a healthy dose of the sun daily.
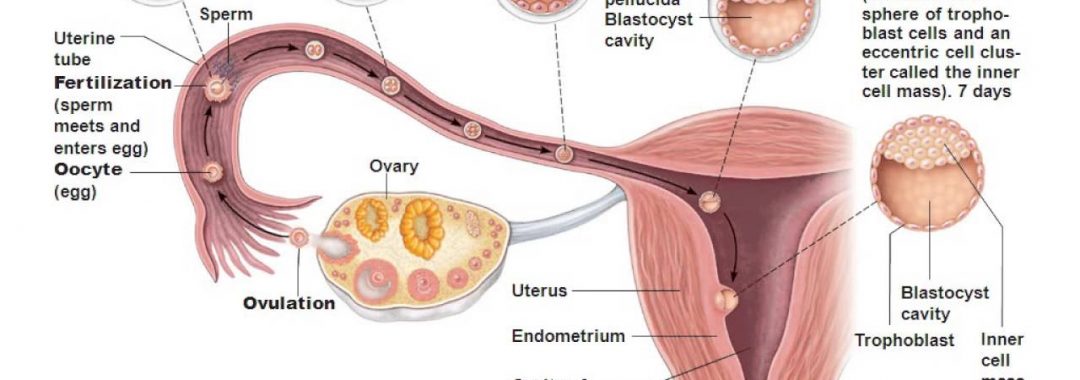
Infertility, or what we call sub-fertility, is becoming an increasing problem and affects millions of people worldwide. More and more people have to turn to assisted reproduction therapy (ART) which now means more and more people are having to use IUI, IVF and ICSI.
The problem is that even with assisted reproduction therapy (ART), at best the success rates are only around 25- 30% on average, and that depends on the clinics individual success rates. Some clinics are also inflating and bodgying success rates to bring in unsuspecting customers.
While there has been much advancements in assisted reproduction (ART) such as IVF and improvements in success rates, the success rates not increased a great deal.
This is why couples need to look at all options and look at preconception care to help increase those success rates. This is why I have set up a fertility program to help educate a couple and assist a couple in everything they need to do in order to increase their chances of a health pregnancy. Couples need to look at a multimodality approach to increasing their chances of conception and this is something is also part of the fertility program.
I often explain to couples that it is like preparing for a marathon; because that is what doing ART can be like. You need to prepare the body (both the man and woman), get the right diet, get the right nutrients, prepare mentally, prepare physically and basically get the bodies into the best shape possible to give the best success. Nobody should ever run a marathon without adequate preparation and the same goes for assisted reproduction.
Vitamin D and reproduction
Researchers across the board know that there is room for improvement in ART success rates. A range of potential factors are being explored, and some scientists have turned their attention to the potential role of vitamin D. While vitamin D is something that needs to be explored, and something that I give to my patients, it needs to be combined with other things mentioned above. It isn’t just as simple as taking Vitamin D and all your fertility problems are gone. But, it is one of the things that can help increase your overall success rates and should be used.
Most of our vitamin D supply is generated in our skin after exposure to sunlight. We do get some from our diets as well. This means that individuals who live in colder or darker environments are more susceptible to lower vitamin D levels, or those who regularly wear clothes covering the majority of their skin, and those who rarely go outside.
The problem these days, many of us have jobs that require us to be inside most of the time and therefore were aren’t getting enough sunlight. The current figures actually show that up to 97% of Australians, and most probably other countries like the US are the same, are actually vitamin D deficient.
The other issue is that even though some of us do get out in the sun, it actually needs to be at a certain time of the day, for optimal absorption. The optimal times are 10am and 2pm in the afternoon. The thing is, most of us aren’t getting out in the sun at these times.
A link between vitamin D and fertility has been theorized for many years and based on a number of observations and studies. This is one of the reasons I have been promoting the use of Vitamin D for more than 20 years now, for those who are on my fertility program. For instance, vitamin D receptors and enzymes have been found in the endometrium.
This is why Vitamin D may be beneficial for women with gynaecological issues such as endometriosis, adenomyosis and other gynaecological conditions.
Vitamin D deficiency has been shown to increase the risk of pre-eclampsia, pregnancy-induced hypertension, gestational diabetes, and lower birth weight. Vitamin D is also essential for a health immune system and reducing inflammation in the body too. It also helps with bone health.
We have also seen that in animal studies, vitamin D deficiency causes poorer fertility and reduced function of the reproductive organs. Many of our breakthroughs in medical science, actually come from animal studies first, especially when it comes to ART and IVF. Many cows and other animals are now impregnated using ART and advancements in this area have helped with human studies.
Vitamin D deficiency and lower success rates
Getting back to the feature studies, Vitamin D was shown to help women undergoing IVF, or intracytoplasmic sperm injection (ICSI), frozen embryo transfer, or both.
All the participants’ vitamin D levels were checked by blood test. What people need to know is that many of the reference ranges still used are actually under review and that if levels of vitamin D in the blood are under 100 Nmols\L, then you need to be supplementing. Anything under 75 Nmols/L is actually deficiency in vitamin D.
This analysis of the current research showed that when women, who underwent ART and had adequate vitamin D levels, were “one third’ more like to have a successful live birth compared to those who were deficient. When compared with women who had insufficient vitamin D concentrations, those with sufficient amounts were “46 percent more likely” to have a clinical pregnancy, and “34 percent more likely” to have a positive pregnancy test result.
Vitamin D is something that I promote and all of my fertility patients are on, as well as other beneficial supplements, diet, emotional support, and medicines etc.
Before you run off trying to buy vitamin D just remember it is just one thing that can help, and it isn’t a miracle cure, but, it may help.
Lastly, before using any supplementations, please consult with a qualified healthcare professional and please don’t self-prescribe, or buy products of the internet. Make sure you buy practitioner dispensed supplements only, which are known to be of the highest quality and not filled with all sorts of things such as heavy metal, low levels of arsenic, toxic fillers etc, which is what some supplements off the internet can have.
Regards
Andrew Orr
-No Stone Left Unturned
-Women’s and Men’s Health Advocate
-The International Fertility Experts
References
- . For the Environment and Reproductive Health Study Team. Serum 25-hydroxyvitamin D concentrations and treatment outcomes of women undergoing assisted reproduction. Am J Clin Nutr. 2016; 104 :729–35.